


Comparison of Continuous Renal Replacement Therapy (CRRT) and Intermittent Hemodialysis (IHD) vs SLEED
Convective Clearance vs Diffusive Clearance

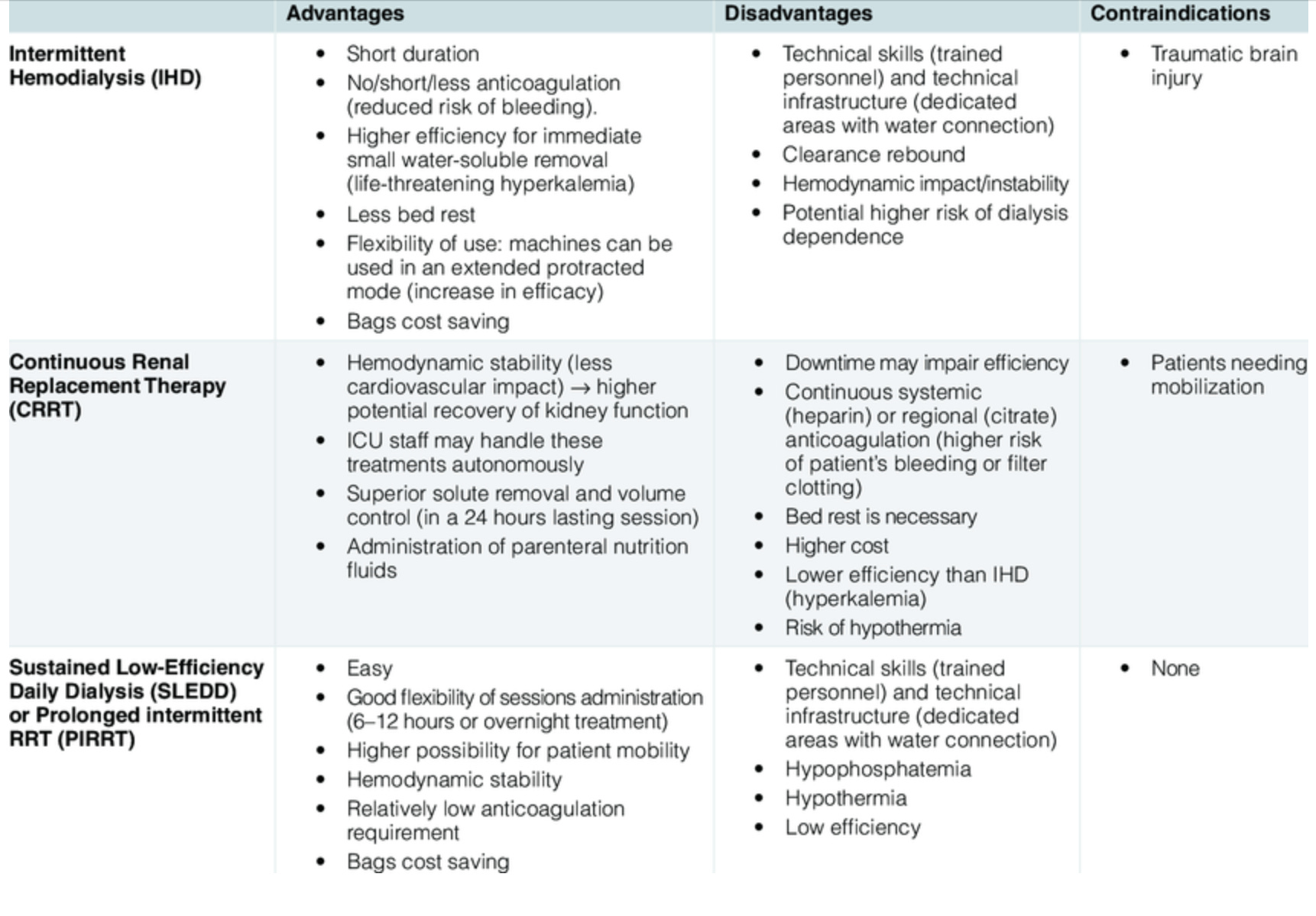
## Comparison of Continuous Renal Replacement Therapy (CRRT) and Intermittent Hemodialysis (IHD)
Continuous renal replacement therapy (CRRT) and intermittent hemodialysis (IHD) are two primary modalities for renal replacement therapy (RRT) used in patients with acute kidney injury (AKI). Both methods have unique characteristics, advantages, and disadvantages that influence their application in clinical settings.
### Efficacy and Outcomes
1. **Survival Rates**: Recent studies indicate that there is no significant difference in survival rates between CRRT and IHD for patients with severe AKI. A meta-analysis involving 1,740 patients found similar short-term mortality and renal recovery outcomes between the two modalities[4]. Additionally, a secondary analysis of multicenter trials showed that patients receiving CRRT had a higher death rate at 60 days compared to those on IHD, particularly in less severely ill patients[1].
2. **Renal Recovery**: Both CRRT and IHD show comparable efficacy in promoting kidney recovery. Studies have consistently demonstrated no significant differences in the rates of dialysis dependency after 30 days between the two groups[3][4].
3. **Length of ICU Stay**: Interestingly, patients undergoing CRRT often experience shorter lengths of ICU and hospital stays compared to those receiving IHD, which may suggest a more efficient management of fluid overload and metabolic derangements[4].
### Mechanisms and Characteristics
| Feature | Continuous Renal Replacement Therapy (CRRT) | Intermittent Hemodialysis (IHD) |
|--------------------------------|---------------------------------------------|----------------------------------|
| **Duration** | Continuous (24 hours) | 3-4 hours, 3 times per week |
| **Blood Flow Rate** | 150-200 mL/min | 300-400 mL/min |
| **Hemodynamic Stability** | Generally good | Poor; hypotension common |
| **Anticoagulation Needs** | Important to prevent filter clotting | Usually not needed |
| **Efficiency** | Lower clearance rate but continuous removal | High clearance rate |
| **Access Type** | Vascular access only | Fistula or vascular catheter |
### Clinical Considerations
- **Patient Selection**: CRRT is often favored in critically ill patients who are hemodynamically unstable due to its ability to maintain better blood pressure control and reduce the risk of hypotension. In contrast, IHD may be more suitable for stable patients who can tolerate the intermittent nature of treatment[2][5].
- **Logistical Factors**: CRRT requires continuous monitoring and is resource-intensive, which can limit its availability in some settings. IHD, while technically simpler, can lead to complications such as dialysis disequilibrium syndrome due to rapid shifts in fluid and electrolytes[2].
### Conclusion
The choice between CRRT and IHD should be guided by patient-specific factors, including hemodynamic stability, severity of kidney injury, and logistical considerations within the healthcare setting. Current evidence suggests that neither modality has a clear superiority regarding survival or renal recovery outcomes; however, individual patient needs may dictate the optimal choice for RRT. Future research is warranted to further clarify these relationships and improve treatment protocols for AKI management.
Citations:
[1] https://pubmed.ncbi.nlm.nih.gov/35379300/
[2] https://litfl.com/ihd-vs-crrt-vs-sled/
[3] https://jtd.amegroups.org/article/view/9206/html
[4] https://onlinelibrary.wiley.com/doi/10.1155/2023/8688974
[5] https://www.cochrane.org/CD003773/RENAL_intermittent-versus-continuous-renal-replacement-therapy-for-acute-renal-failure-in-adults